Most “wellness” devices on the market are little more than expensive desk lamps that fail to reach the biological depth required for systemic relief. Are you tired of relying on a cycle of NSAIDs or topical treatments that barely scratch the surface of your discomfort? We understand the frustration of navigating a marketplace filled with conflicting technical specs and unverified claims. You deserve a solution grounded in light physics, not marketing hype. Using red light therapy for chronic pain is only effective when the device delivers sufficient irradiance to reach deep-seated joints and nerves.
This clinical guide establishes a rigorous framework for using photobiomodulation to manage persistent physical distress. You’ll discover how to select lab-verified devices that actually reach deep tissue, ensuring your investment leads to a measurable reduction in daily pain scores and improved mobility. We’ll unpack the critical role of the 850nm and 1064nm wavelengths and explain why a minimum irradiance of 100mW/cm² at six inches is often non-negotiable for therapeutic success. By the end of this deep dive, you’ll have the technical literacy to distinguish between FDA-cleared medical tools and ineffective consumer gadgets, providing a clear path toward evidence-based recovery.

Key Takeaways
- Understand the biological process of photobiomodulation and how light-tissue interactions at the cellular level can interrupt persistent pain signals.
- Identify why the “optical window,” specifically near-infrared and 1064nm spectra, is essential for reaching deep-seated tissue and bone.
- Learn to evaluate device efficacy by prioritizing irradiance (mW/cm²) over total wattage to ensure your panel has the power density to be effective.
- Apply clinical protocols to calculate precise dosing, avoiding the “more is better” fallacy that can diminish the benefits of red light therapy for chronic pain.
- Access lab-verified recommendations for 2026 to select modular, high-irradiance devices that meet rigorous clinical standards for safety and performance.
The Biological Mechanism: How Photobiomodulation Interrupts Chronic Pain


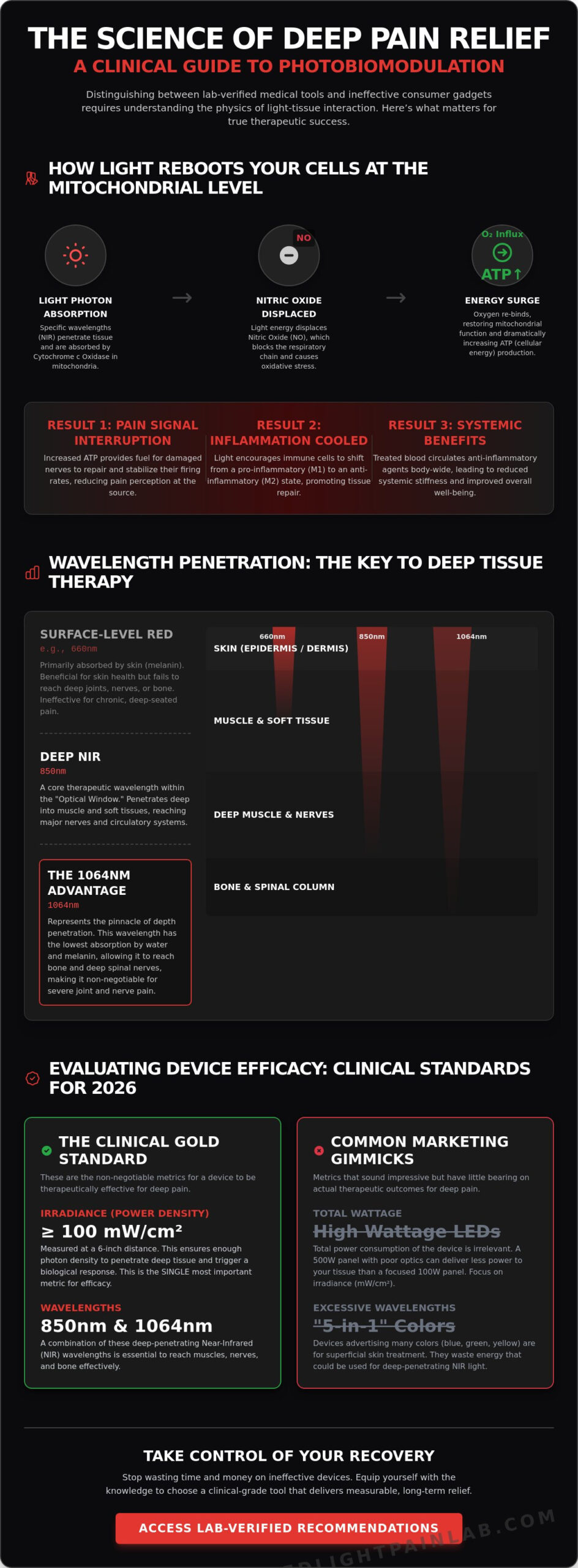
Why does a specific wavelength of light have the power to alter a long-standing pain signal? The answer lies not in heat, but in a precise biological interaction known as Photobiomodulation (PBM). Unlike surgical lasers that cut or cauterize tissue, PBM utilizes non-thermal light to trigger a photochemical response within the mitochondria. This is the foundation of using red light therapy for chronic pain. When photons of light reach the cellular level, they are absorbed by a specific protein called Cytochrome c Oxidase. This enzyme acts as the primary photo-acceptor, initiating a cascade of events that changes how your cells produce energy and process damage.
Mitochondrial Optimization and the ATP Surge
When your tissues are chronically inflamed, Nitric Oxide (NO) often binds to Cytochrome c Oxidase, effectively clogging the cellular engine and halting respiration. Light therapy physically displaces this Nitric Oxide. This allows oxygen to rush back in, restarting the production of Adenosine Triphosphate (ATP). Increased ATP provides the necessary fuel for nociceptors, our pain-sensing nerves, to repair their damaged membranes and stabilize their firing rates. ATP is the currency of cellular healing in pain management. This surge in energy doesn’t just mask the sensation; it provides the biological resources required to fix the underlying structural dysfunction.
Cytokine Modulation: Cooling the Fire of Chronic Inflammation
Chronic pain is often a result of a self-perpetuating inflammatory cycle. In these states, macrophages, which are specialized immune cells, often get stuck in an M1 pro-inflammatory state. Exposure to near-infrared light encourages these cells to shift into an M2 anti-inflammatory state, which promotes tissue remodeling and repair. This shift reduces the oxidative stress that typically degrades cartilage and joint lining. It also addresses the “wind-up” phenomenon, a condition where the central nervous system becomes hypersensitive to pain stimuli. By cooling this internal fire, light therapy helps reset the baseline of the nervous system. This transition is vital for those who have found traditional anti-inflammatories to be ineffective.
Does treating a single joint benefit the rest of the body? Research suggests it does. As blood flows through the treated area, it carries light-activated signaling molecules and anti-inflammatory cytokines throughout the vascular system. This systemic effect means that localized red light therapy for chronic pain can contribute to a broad reduction in full-body inflammation, providing relief that extends beyond the immediate target site. This interconnected response is why many users report improved sleep and reduced systemic stiffness even when targeting a specific injury.
Wavelength Depth: Why 1064nm and NIR are Essential for Deep Tissue
Why do so many users fail to see results when using red light therapy for chronic pain? The answer is often a failure of physics rather than a failure of the technology itself. For light to trigger a biological response, it must first reach the target tissue. The human body possesses an “Optical Window” between 600nm and 1100nm. Within this specific range, light can penetrate the skin and soft tissue without being immediately absorbed by water or hemoglobin. If your device operates outside these parameters, the energy is wasted at the surface, never reaching the deep-seated nerves or joints causing your distress.
Spectroscopic analysis reveals that different wavelengths face different obstacles. Melanin in the skin is a primary absorber of shorter wavelengths, while water in our cells begins to block light as it moves deeper into the infrared spectrum. Understanding this balance is critical. Brown University Health explains photobiomodulation as a process of mitochondrial stimulation; however, that stimulation is impossible if the photons are trapped in the dermis. This is why a clinical approach requires a move beyond simple “red” light into the more powerful near-infrared (NIR) spectrum.
The 1064nm Advantage: Reaching the Bone and Deep Nerves
The 1064nm wavelength represents the new frontier in managing deep-seated physical discomfort. Unlike the standard 850nm wavelength, 1064nm has a significantly lower absorption coefficient in water. This allows the light to travel through the body’s aqueous environment with less resistance, reaching depths that were previously inaccessible to consumer devices. For patients dealing with spinal issues, deep hip joint inflammation, or radiculopathy, 1064nm is often the missing link. Clinical evidence suggests that this wavelength is particularly effective for treating neuropathy, as it can reach the deep nerve bundles that 850nm might only graze. If you are targeting structural issues deep within the body, it’s vital to investigate lab-verified panels that include this specific spectral output.
660nm vs. 850nm: Balancing Surface and Subsurface Relief
Don’t mistake depth for the only metric of success. A comprehensive strategy requires a multi-layered approach. The 660nm wavelength is a powerhouse for superficial concerns, such as tendonitis in the hands or skin-level inflammation. It stops largely at the dermis, providing high-intensity energy to the most accessible tissues. Conversely, 850nm remains the workhorse for muscle recovery and joint capsule pain. It penetrates the muscle belly, facilitating the ATP surge discussed in previous sections. The most effective devices utilize a synergistic blend of these wavelengths. By combining 660nm, 850nm, and 1064nm, you ensure that every layer of tissue, from the skin to the bone, receives the therapeutic irradiance necessary for long-term relief.
Evaluating Device Efficacy: Irradiance and Power Density Standards
Why do consumer “beauty” wands fail to impact deep joint pain? They lack the power density required to penetrate human tissue. Irradiance, measured in milliwatts per square centimeter (mW/cm²), is the only metric that determines the true “punch” of a panel. While manufacturers often highlight total wattage, this figure is often a deceptive marketing gimmick. Total wattage refers to the power the device consumes from the wall, not the therapeutic energy delivered to your body. If a manufacturer refuses to provide irradiance data, it’s a clear signal that the device is underpowered for clinical use.
The “Distance Decay” problem further complicates this measurement. As you move away from a light source, the intensity of that light drops off precipitously. A panel might boast high power at the surface, but those numbers can plummet by 50% or more just six inches away. This is why standardized testing distances are non-negotiable for anyone using red light therapy for chronic pain. Without verified irradiance data at specific distances, you’re essentially guessing your dose. We prioritize panels that maintain high power density across a broad treatment area, ensuring consistent results.
The Irradiance Threshold for Deep Tissue Pain
To achieve clinical results for structural issues, a minimum irradiance of 100 mW/cm² at a 6-inch distance is generally required. Anything less may provide superficial benefits but will fail to reach the mitochondrial targets in deep joints or the spine. When evaluating a device, always demand a 3rd-party lab report featuring spectroradiometer data rather than relying on manufacturer claims. Remember that visible brightness is not an indicator of NIR power; since near-infrared light is invisible to the human eye, the most therapeutic wavelengths won’t look “bright” at all.
EMF and Flicker: Protecting the Nervous System
High-power electronic devices naturally generate electromagnetic fields (EMF). Patients suffering from chronic pain often exhibit heightened central nervous system sensitivity, making them more vulnerable to the bio-effects of high EMF exposure. Similarly, poor-quality LED drivers can cause light flicker. While often invisible, this rapid pulsing can trigger headaches or eye strain by overstimulating the ocular nerves and brain. Our investigative process prioritizes verification. We look for devices that utilize high-quality drivers to ensure zero-EMF and flicker-free performance, protecting your nervous system during recovery.
Clinical Protocols: Dosing and Positioning for Long-Term Relief
How do you determine the exact point where light stops being therapeutic and starts being inhibitory? This challenge is defined by the Arndt-Schulz Law, which describes a biphasic dose-response. In clinical photobiomodulation, a low dose provides a stimulating effect, while an excessively high dose can actually suppress cellular function. This is why “more light” is not always a better solution for physical distress. To establish an effective protocol for using red light therapy for chronic pain, you must move beyond guesswork and utilize a mathematical approach to dosing. The standard therapeutic window for deep tissue pain typically falls between 15 and 60 Joules per square centimeter (J/cm²).
Calculating your dose requires a simple but essential formula: (Irradiance in mW/cm² x Time in seconds) / 1000 = Joules/cm². If you are using a high-irradiance panel that delivers 100 mW/cm² at six inches, a ten-minute session results in a dose of 60 J/cm². Positioning is equally critical. For lower back pain, a large modular panel should be positioned to cover the entire lumbar region, ensuring the light penetrates the deep muscle layers and spinal discs. Knee arthritis requires a more targeted approach, often involving a wrap or a panel angled to reach the joint capsule from multiple sides. For systemic conditions like fibromyalgia, full-body exposure is necessary to trigger the systemic anti-inflammatory effects discussed in previous sections.
The 10-20-6 Rule: A Universal Starting Point
A 10-20 minute exposure at a 6-inch distance serves as a reliable baseline for most clinical-grade panels. This distance ensures you receive high irradiance while allowing for a slight buffer to prevent heat buildup on the skin. If the pain site is particularly sensitive or acute, you might start at 12 inches to lower the intensity before gradually moving closer as your tolerance improves. Watch for signs of over-dosing, such as temporary fatigue or a slight increase in sensitivity at the treatment site. These are biological signals that the tissue has reached its saturation point. To find a device that meets these power requirements, you can compare lab-verified red light therapy panels that provide transparent irradiance data.
Frequency and Consistency: Building the Cumulative Effect
Why are daily sessions superior to sporadic, high-intensity treatments? The biological benefits of light therapy are cumulative. Each session builds upon the cellular energy surge of the previous day, gradually lowering the baseline of inflammation. Most clinical observations suggest a “loading phase” of 4 weeks, where daily use is required to see significant shifts in daily pain scores. Once you achieve your desired outcome, you can transition to a “maintenance phase” of 3-4 sessions per week. Integrating red light therapy for chronic pain with gentle physical therapy or stretching can yield synergistic results, as the increased ATP production provides the fuel needed for more effective movement and rehabilitation.
Selecting the Optimal Panel: Lab-Verified Recommendations for 2026
How do you navigate a marketplace saturated with underpowered consumer electronics? You prioritize technical verification over aesthetic marketing. Selecting a device for red light therapy for chronic pain requires a commitment to data, specifically third-party spectroradiometer reports that confirm wavelength precision. We advocate for modular systems because they offer a scalable solution for evolving health needs. If you begin by treating a localized joint injury but later require spinal coverage, modularity allows you to link panels together without discarding your initial investment. This structural flexibility is a hallmark of a professional-grade setup.
A five-year warranty is a critical indicator of industrial-grade components. High-irradiance panels generate significant heat; inferior cooling systems lead to diode degradation and a loss of therapeutic power over time. We look for manufacturers that provide clinical power while maintaining the low EMF and flicker-free performance established in our safety standards. By using our curated discount codes, you can access this clinical-grade technology without the typical markup found in medical-only distribution channels. This value analysis ensures you pay for light physics, not a brand’s advertising budget.
Best Full-Body Panels for Systemic Inflammation
Does your condition involve systemic inflammation, such as fibromyalgia or autoimmune-driven discomfort? Full-body coverage is essential for these cases. Large arrays ensure that the blood flowing through your vascular system is consistently exposed to the light, triggering a body-wide anti-inflammatory response. In the 2026 market, the most effective units utilize advanced heat sinks and quiet-run fans to ensure the power draw remains stable during 20-minute sessions. For many users, particularly those focusing on red light therapy for chronic pain in the lower back, “half-body” panels represent the ideal balance of high irradiance and affordability.
Targeted Devices for Peripheral Neuropathy and Joint Pain
Precision often outweighs sheer size when treating localized nerve issues. If you are managing peripheral neuropathy in the feet or hands, a small, high-intensity panel allows for closer positioning and higher power density. We specifically prioritize recommendations for devices that integrate dedicated 1064nm chips. As established in our depth analysis, this wavelength is vital for reaching the deep-seated nerves that standard 850nm diodes might miss. A targeted device is often more practical for those who need to maintain a strict daily protocol while traveling or working.
Before making a final decision, verify that your chosen device meets the 100mW/cm² threshold at your intended treatment distance. This technical literacy protects you from “beauty” devices that lack the biological efficacy required for recovery. To streamline your selection, review our top 5 clinical-grade panels here. This final checklist ensures your chosen hardware matches the rigorous protocols outlined in this guide, moving you closer to a future with reduced daily pain scores.
Transitioning from Passive Relief to Active Cellular Healing

Will you continue to rely on temporary topical solutions, or is it time to address the mitochondrial root of your discomfort? We have established that successful red light therapy for chronic pain is a matter of precise light physics. By prioritizing deep-penetrating 1064nm wavelengths and maintaining an irradiance threshold of at least 100 mW/cm², you move beyond the surface-level limitations of standard consumer devices. Remember that consistency and calculated dosing are your most effective tools for resetting the nervous system and cooling systemic inflammation.
The marketplace is crowded with unverified claims, but you don’t have to navigate it alone. We have performed the technical heavy lifting by providing independent lab verification of irradiance and wavelengths for the industry’s leading hardware. You can view our lab-tested rankings of the best red light therapy panels for pain, where we offer a detailed comparison of 50+ clinical-grade panels and exclusive discount codes for top-tier brands. Armed with this scientific framework, you are now equipped to choose a device that delivers measurable biological results. Sustainable relief is a journey of precision, and you have already taken the most important step toward recovery.
Frequently Asked Questions
Is red light therapy safe for eyes when treating facial pain?
Eye protection is mandatory when using high-irradiance panels for facial pain. While the light is non-ionizing, the sheer intensity of clinical-grade LEDs can cause significant ocular strain and glare. Standard safety protocols recommend using opaque or specific wavelength-filtering goggles. Closing your eyes is insufficient protection against the power density required for therapeutic tissue penetration, and prolonged exposure without shielding may lead to temporary vision disturbances.
Can I use red light therapy if I have a metal implant or pacemaker?
Red light therapy is generally safe for individuals with metal implants because it utilizes non-thermal light energy. Unlike microwave or ultrasound therapies, it doesn’t cause significant heating of metallic structures within the body. However, if you have an active implanted device like a pacemaker, you must consult your cardiologist. While the light itself is safe, the electronic drivers in high-power panels can generate electromagnetic fields that may interfere with sensitive electronics.
How long does it take for red light therapy to work for chronic back pain?
Most users observe a measurable reduction in daily pain scores after a consistent four-week loading phase. While some individuals experience acute relief after a single session due to immediate Nitric Oxide displacement, lasting results for red light therapy for chronic pain require cumulative cellular repair. Chronic back pain involves deep structural issues that necessitate regular mitochondrial stimulation over several weeks to alter the underlying inflammatory baseline.
What is the difference between red light therapy and a heating pad?
A heating pad relies on conductive heat to increase surface blood flow, whereas red light therapy triggers a photochemical reaction at the cellular level. Heating pads provide temporary symptomatic relief by relaxing muscles, but they cannot stimulate ATP production or repair damaged tissue. Light therapy utilizes specific wavelengths to penetrate deep into the joint capsule, addressing the biological cause of the pain rather than just masking the sensation with warmth.
Do I need to wear clothes during my red light therapy session?
Direct skin exposure is essential because photons cannot effectively penetrate most clothing materials. Fabrics reflect or absorb the light energy, preventing the necessary irradiance from reaching your target tissues. For maximum therapeutic efficacy, the treatment area should be completely bare. If you are treating systemic inflammation with a full-body panel, minimal clothing or nudity ensures that the maximum surface area is available for light-tissue interaction.
Can red light therapy help with nerve pain and neuropathy?
Clinical research indicates that red light therapy for chronic pain is highly effective for peripheral neuropathy and radiculopathy. Near-infrared wavelengths, particularly the 1064nm spectrum, reach the deep nerve bundles to stimulate axonal regeneration and reduce oxidative stress. This process helps stabilize the firing rate of nociceptors, leading to a significant decrease in the burning or tingling sensations often associated with chronic nerve damage.
What happens if I use red light therapy for too long in one session?
Exceeding recommended session times can lead to a phenomenon known as the biphasic dose-response, where the light actually inhibits cellular healing. If you over-dose the tissue, you may experience temporary lethargy, a slight headache, or a transient increase in pain sensitivity. This occurs because the mitochondria have reached their saturation point and can no longer process the incoming photons, leading to a temporary stall in cellular respiration.
Is it better to use red light therapy in the morning or at night for pain?
Morning sessions are often superior for managing the stiffness and discomfort associated with waking up, as they provide an immediate ATP surge for daily mobility. Conversely, using the therapy at night can support the body’s natural repair cycle during sleep and may help regulate circadian rhythms. The most critical factor is consistency; choose a time that allows you to maintain your protocol without interruption to ensure cumulative results.